Aug 25, 2016 | Research Updates

Stephen V Faraone, Ph. D Director of Medical Genetics Research and Professor in theDepartments of Psychiatry and Neuroscience & Physiology at SUNY Upstate Medical University
We know from many studies that ADHD is associated with a slightly lower intelligence quotient (IQ) and with problems in thinking known as executive function deficits. If that’s that case, you might think that people with a high IQ cannot have ADHD. You would be wrong. Data on groups sometimes mislead us about individuals. Although, on average, ADHD people have IQ scores that are about 9 points lower than others, there is a wide spread of IQs in both ADHD and non-ADHD people. So many people with ADHD have higher IQs than those without ADHD and vice-versa. Moreover, studies of people with high IQs support the idea that ADHD can be validly diagnosed among very intelligent individuals.
In a series of studies using the, Antshel and colleagues showed that the clinical profile of high IQ ADHD was very similar to what has been observed for ADHD in general. For example, like their less intelligent counterparts, high IQ ADHD children have an increased risk for mood, anxiety and disruptive behavior disorders. Children with a high IQ and ADHD showed a pattern of familial transmission as well as cognitive, psychiatric and behavioral impairments consistent with the diagnosis of ADHD. The degree to which ADHD persisted into adulthood was also similar between the two groups.
In studies of adults with ADHD, the same group concluded that “adults with ADHD and a high IQ display patterns of functional impairments, familiality and psychiatric co-morbidities that parallel those found in the average-IQ adult ADHD population.” Of particular interest, despite their high intelligence, High-IQ adults with ADHD show impaired executive functioning and their performance on tests of executive functioning predicted life impairments.
Why are these data important? Milioni and colleagues argue that among higher IQ adults with ADHD, a higher degree of intellectual efficiency may compensate for deficits in executive functions. This ability to compensate allows them to succeed in many tasks which otherwise might have been impaired by their ADHD symptoms. But, in many cases, such compensation is not sufficient or is too burdensome. When compensation fails, ADHD symptoms and other impairments emerge. When this occurs later in life, some clinicians are reluctant to diagnose ADHD. Caution is warranted, but clinicians need to know that the diagnosis of ADHD among high IQ is valid.
References:
Antshel, K. M., S. V. Faraone, et al. (2008). “Temporal stability of ADHD in the high-IQ population: results from the MGH Longitudinal Family Studies of ADHD.” J Am Acad Child Adolesc Psychiatry 47(7): 817-825.
Antshel, K. M., S. V. Faraone, et al. (2009). “Is adult attention deficit hyperactivity disorder a valid diagnosis in the presence of high IQ?” Psychol Med 39(8): 1325-1335.
Antshel, K. M., S. V. Faraone, et al. (2010). “Executive functioning in high-IQ adults with ADHD.” Psychol Med 40(11): 1909-1918.
Antshel, K. M., S. V. Faraone, et al. (2007). “Is attention deficit hyperactivity disorder a valid diagnosis in the presence of high IQ? Results from the MGH Longitudinal Family Studies of ADHD.” J Child Psychol Psychiatry 48(7): 687-694.
Katusic, M. Z., R. G. Voigt, et al. (2011). “Attention-deficit hyperactivity disorder in children with high intelligence quotient: results from a population-based study.” J Dev Behav Pediatr 32(2): 103-109.
Mar 31, 2016 | Research Updates
ADHD and Negative Thinking
Cognitive-behavioral therapy (CBT) is a psychosocial treatment that has been adapted for use with adults with ADHD. Numerous clinical outcome studies, including several randomized trials comparing Cognitive Behavioral Therapy (CBT) with active control treatments have yielded positive results, often in combination with ADHD medications.
A common element in most CBT approaches for adult ADHD is the focus on behavioral skills training. ADHD is an implementation problem inasmuch as individuals describe being aware of what needs to be done to manage the effects of ADHD (not to mention other areas of life) but yet have difficulties consistently and effectively performing these skills. In fact, there has been some question as to whether the cognitive element of CBT – identifying and modifying maladaptive thoughts – is really essential in the treatment of adult ADHD apart from their relevance in cases of co-existing anxiety and depression.
 However, several recent studies have started to identify the unique impact of negative thinking on adults with ADHD. These studies have illustrated that dysfunctional attitudes and cognitive-behavioral avoidance overlapped to contribute to co-existing depression and depressive symptoms1, are more prominent in cases of ADHD and co-existing depression but are also more prominent in cases of uncomplicated ADHD when compared to controls2, and uncomplicated ADHD was associated with higher levels of intrusive and worrisome thoughts when compared with controls3.
However, several recent studies have started to identify the unique impact of negative thinking on adults with ADHD. These studies have illustrated that dysfunctional attitudes and cognitive-behavioral avoidance overlapped to contribute to co-existing depression and depressive symptoms1, are more prominent in cases of ADHD and co-existing depression but are also more prominent in cases of uncomplicated ADHD when compared to controls2, and uncomplicated ADHD was associated with higher levels of intrusive and worrisome thoughts when compared with controls3.
More recently, a chart review study of 44 adults assessed the correlation of ADHD with measures of self-reported distorted thoughts, depression, anxiety, and hopelessness4. A significant, positive correlation between distorted thoughts and a measure of ADHD was obtained; there was no correlation between ADHD and depression, anxiety, or hopelessness. Review of the most frequently endorsed categories of cognitive distortions indicated that “Perfectionism” (55%) was far and away the most frequently endorsed, followed by “Emotional Reasoning and Decision-Making” (17.5%, “Comparison to Others” and “Emotional Reasoning” (both 7.5%).
The combinations of findings indicate that the cognitive component of CBT is still relevant in helping adults with ADHD to better implement various effective behavioral coping strategies in their daily lives. The aforementioned distortions play a role in the cognitive-behavioral avoidance identified in the various other studies of negative thoughts and adult ADHD. Distorted cognitions are central to procrastination, emotional management, problem-solving, and various other coping domains commonly targeted in psychosocial treatment. Thus, although the implementation of behavioral skills in order to improve overall functional status and well-being are an important outcome of CBT for adult ADHD, it is increasingly appreciated that cognitive interventions play a central role in achieving these outcomes.
1 Knouse, L. E., Zvorsky, I., & Safren, S. A. (2013). Depression in adults with attention-deficit/hyperactivity disorder (ADHD): The mediating role of cognitive-behavioral factors. Cognitive Therapy & Research. 37, 1220-1232. doi: 10.1007/s10608-013-9569-5
2 Mitchell, J. T., Benson, J. W., Knouse, L. E., Kimbrel, N. A., & Anastopoulous, A. D. (2013). Are negative automatic thoughts associated with ADHD in adulthood? Cognitive Therapy and Research, 37, 851-859. doi: 10.1007/s10608-013-9525-4
3 Abramovitch, A., & Schweiger, A. (2009). Unwanted intrusive and worrisome thoughts in adults with Attention Deficit/Hyperactivity Disorder. Psychiatry Research, 168, 230-233. doi:10.1016/j.psychres.2008.06.004
4 Strohmeier, C., Rosenfield, B., DiTomasso, R.A., & Ramsay, J. R. (2016). Assessment of the relationship between cognitive distortions, adult ADHD, anxiety, depression, and hopelessness. Psychiatry Research, 238, 153-158. doi: 10.1016/j.psychres.2016.02.034
Feb 14, 2016 | Research Updates
ADHD and Bipolar Disorder in Children
 Joseph L. Biederman, MD
Joseph L. Biederman, MD
Over the last twenty years, since the 1990’s, there has been an increasing awareness in pediatric psychiatry that a sizable number of children, probably around one percent, have Bipolar illness. This is also supported by the fact that roughly seventy percent of adults with Bipolar illness start their illness in childhood and adolescence. We face a real problem that somewhere about one percent of children may be affected.
The problem in the field of ADHD and Bipolar illness is that about eighty percent of children with Bipolar illness also have ADHD. It’s not in reverse. The rate of Bipolar illness in children with ADHD is around twenty percent. The overlap is quite substantial, but particularly very, very high in children with Bipolar illness.
The reason this is important is because ADHD and Bipolar in children may share some symptoms, but they require very different treatments. The treatments that we use for ADHD can make worse the symptoms of bipolarity. Particularly if we use medicines like stimulants, or medicines like anti-depressants.
So these things are very consequential to the well-being of the child. Children with Bipolar illness frequently are violent, aggressive, and can be out of control. Very often they are so out of control that they need to be hospitalized. They become dangerous to self or others. So the differential diagnosis of ADHD from Bipolar illness has enormous clinical and therapeutic consequences.
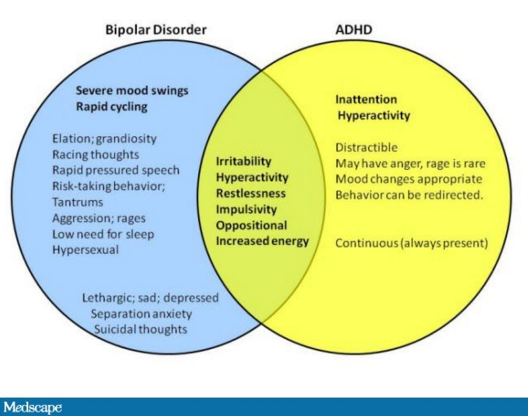
There are shared symptoms in common between ADHD and Bipolar Disorder, but they are different. Hyperactivity and agitation are not exactly the same. Hyperactive children move a lot, but they are not in an agitated state. Children with ADHD tend to talk a lot, but children with Bipolar illness talk so rapidly that sometimes they cannot be understandable.
But the major differentiation is in the abnormal mood. There is nothing in the defining features of ADHD that speak to abnormal mood. Bipolar children have very, very dysregulated mood. They frequently have the combination of aggression, manic symptoms, and depression all at the same time.
It’s a very complicated clinical picture that is usually known as mixed mania. Children with mania, more often than not, tend to be irritable, violent, and aggressive, not euphoric. The children present usually at a very young age, usually with symptoms of dyscontrol, and violence. Very often the symptoms present at home for a long time, before they spread to the school. Because when the symptoms emerge in the school, the child becomes unmanageable and usually is brought to the emergency room.
Despite the fact that some symptoms overlap, there are very, very important differentiating features between ADHD and Bipolarity. Remember I said before that eighty percent of children with Bipolar illness also have ADHD. The ADHD that they have is going to be very severe. But they also have mood dysregulation, irritability, and sometimes violent behaviors.
It is very important for clinicians and parents to learn how to distinguish ADHD from Bipolar Disorder, and treat each appropriately, particularly because of their high comorbidity. ADHD and Bipolar in adults can be similarly challenging, but here we have the maturity of adults who can better describe their symptoms.
Feb 8, 2016 | Research Updates
ADHD Genes Found
Stephen V. Faraone, PhD
For many years, ADHD scientists have been searching for genes that pre-dispose people to having ADHD, a very difficult investigation. It turns out that the solution to the problem of finding genes was in getting large enough samples, so that we had enough statistical power to actually find these genes. What has been created is an international consortium consisting of over 100 people from 14 countries and five continents who are studying the genetics of ADHD. We pooled our data into a very, very large genome-wide association study, then we studied the entire human genome, looking for genes or, I should say, DNA variants.
This is the DNA that puts people at risk for having ADHD. Right now we have about 17,000 ADHD people in this big experiment, along with 95,000 controls. It’s really the largest experiment study in ADHD ever to have been done. What’s really exciting about this in 2016 is that, finally, after many years of doing these genome-wide studies, we can finally say for certain that we have detected loci on these genomes that are what we call genome-wide significant, meaning that we’re very sure that they are pointing to genes that are associated with ADHD. We think we have between five and eight genes that we can be sure about. We’re actually finalizing an analysis. I presented the final results at the January 2016 annual meeting of APSARD, the American Professional Society of ADHD and Related Disorders.
So far, the genes that we’ve discovered are quite interesting, because they’re pointing to novel pathways that haven’t been considered before. For example, everybody knows about the Dopamine system in ADHD and the Norepinephrine system in ADHD. These are well-known biological pathways that have been located by the treatments for the disorder. We’re now locating biological paths which, for example, are involved in synaptic plasticity in the development of the brain. These are genes that are involved both very early on in the brain during development, from the fetal stage up through young adulthood. They are also involved in learning and memory in the remodeling of synapses.
We hope, in the long run, that discovering these new genes and new biological pathways will give us new insights into how medications might be developed to target very specific problems that will occur in the ADHD brain. These are very exciting days for the people who have studied the genetics of ADHD. More importantly, these discoveries will bring exciting new treatments to ADHD patients, their loved ones, and medical professionals.
Feb 4, 2016 | Research Updates
How ADHD Grew Up as Kids Grew into ADHD Adults
 (Editors’s Note: This text comes from transcription of an extensive interview on November 23, 2015 with Ronald C. Kessler, PhD.)
(Editors’s Note: This text comes from transcription of an extensive interview on November 23, 2015 with Ronald C. Kessler, PhD.)
There’s a lot of evidence to show that the structure of ADHD changes from childhood to adulthood. For many years there was a widespread belief that ADHD kind of disappeared, people matured out of ADHD as they got into adulthood. We know now that’s not the case, but as we learn more and more about people who have ADHD as they age, we realize that what seemed to be that “ADHD disappearing” was really a transforming. The kinds of symptoms that people have change, so the hyperactive and impulsive symptoms become less prominent, the inattentive symptoms become more prominent, and also we’re coming to understand now that they’ve become more differentiated. It’s really the symptoms become more of a spectrum of executive dysfunction than just inattentiveness.
There’s also some thinking that there might be another dimension that becomes important, and it’s not just the cognitive part of the executive dysfunction, but some kind of emotional dyscontrol that looks somewhat different from hyperactivity or impulsivity in childhood. We’re interested in looking into that as a way of helping to refine the ADHD diagnostic criteria. As you in know DSM-5 has just been put into place in May, 2013. We looked at the full set of adult ADHD symptoms in the DSM-5, which is the 9 AD and the 9 HD impulsive symptoms. This is in addition to about a roughly equal number of other symptoms that had been suggested by various experts as being indicative of adult ADHD that you don’t see in kids. Again, most of these problems were associated with things having to do with executive function, so trying to manage complex tasks and things that a person might do as an adult worker is different from what a 12-year old child has to deal with.
We also asked about emotional dyscontrol. When we analyzed that, we found a very consistent structure across three surveys. We found clear evidence of one dominant factor that was really not AD (attention deficit symptoms.) It was again, the AD symptoms plus this broader array of executive dysfunction symptoms; not being able to finish tasks on time and juggling multiple tasks, and the kind of things that you and I and other people in the modern world have to deal with all the time.
We found four factors in adult ADHD patients: attention deficit, hyperactivity, impulsivity, emotional dyscontrol. All four of those were very strongly correlated in having a diagnosis leading to DSM-5 ADHD criteria. So we find that these factors are important, but as it turns out, the emotional dyscontrol measure, and the broader executive functioning measures that are not part of DSM-5 have associations with the diagnosis equally as strong as the symptoms that are part of DSM-5. So it’s very clear that the symptoms that are used right now in DSM-5 are really just a subset of a broader set of symptoms in the general population. That’s the first thing we found.
Then we’ve done some other interesting things based on that, looking at the profiles of people, and looking at the kinds of symptoms that seem to be dominant. The question is, is there any evidence to suggest that there is a broader spectrum of ADHD where people who don’t quite make DSM criteria had a large set of other items that should be in the same spectrum, but have been missed then. That’s the basic idea here.
We have DSM-5, which is like the physician’s desk manual for what is classified as ADHD and what is not ADHD in the field of mental disorders. New associations are being found. So what do practitioners do with that before DSM-6 comes out? How does this spread into the population of practitioners who are trying to correctly diagnose people?
 One big purpose of this is forward thinking for DSM-6, which is now quite a ways off since we just started with DSM-5, but it’s important to get straight what the nature of the beast is if you’re trying to get better diagnoses. So we hope that over the next few years we will be looking at the data on the structure of ADHD to be the foundation for deeper studies to help us flesh out sub-types that are more meaningful in adulthood than in childhood. But for the “right now” part, what we’re finding is that even when a person meets current criteria for adult ADHD, the things that are the symptoms in DSM-5 might not be the presenting complaints!
One big purpose of this is forward thinking for DSM-6, which is now quite a ways off since we just started with DSM-5, but it’s important to get straight what the nature of the beast is if you’re trying to get better diagnoses. So we hope that over the next few years we will be looking at the data on the structure of ADHD to be the foundation for deeper studies to help us flesh out sub-types that are more meaningful in adulthood than in childhood. But for the “right now” part, what we’re finding is that even when a person meets current criteria for adult ADHD, the things that are the symptoms in DSM-5 might not be the presenting complaints!
Patients don’t come in to a doctor and say “Gee, I have a problem with things that are half impulsive, and half hyperactive.” Further, the aspects of inattention are very often kid-oriented and do not necessarily present as a problem for adults. It might be that for the doctor, it’s easier to pick up on the syndrome by asking about things that are not current in DSM-5. In terms of screening, the ability to find people who have a problem who don’t realize it yet, get them the treatment that could be helpful and improve the quality of life could be improved by us having a better understanding of what the real life problem is. Because of this, one of the spin-offs of this analysis is that a group of us are working on a revision of the ASRS Screener (ASRS V1.1, the current six question ADHD screener used by clinicians to screen for ADHD: Adult Self-Report Scale) that broadens the set of questions to include executive dysfunction, to see if there is a more diagnostic set of questions that could help us identify ADHD in adults. Then a group of us as well are studying the structural aspect of ADHD to see in clinical research studies if we should be probing a little bit more deeply for sub-types of ADHD where it might make sense to think of differential treatment response, or a treatment response to executive dysfunction in new ways that we haven’t used before.
The most notable is that the emotional dyscontrol set of symptoms don’t seem to be as distinct from the executive dysfunction problems, the way AD and HD are in childhood. It turns out that those emotional characteristics are more prominent in adulthood than we had previously thought when we were looking only at hyperactivity and impulsivity. We have had this conception that ADHD adults are just like tall kids; they have this AD part and they have this HD part. We’ve always known that AD is more prominent, but we now know it’s broader too. It’s really not AD, it’s executive dysfunction, and that’s sort of a richer, more variegated kind of problem.
Instead of it being just hyperactive and impulsive, it’s really hyperactive and impulsive and emotional dyscontrol, where you don’t see so much hyperactivity or impulsivity in adults but rather a more subtle kind of emotional dyscontrol. There are a lot of people as adults who have a combined type of ADHD, as opposed to a pure executive dysfunction problem. But you don’t see the combined aspect of it if all you do is focus on the impulsivity and hyperactivity. Neither of those are so obvious in adults, and you miss the fact there are these more subtle, emotional dyscontrol pieces if you are not looking for them using DSM-5 criteria.
ADHD was originally described in the early 1900’s, and here we are 100 years later, underlining how new this science is and our understandings are. It’s not uncommon to see definitions get carved in stone. There are many medical conditions that are not terribly difficult to study, if you look at them, but they just never get looked at because of pre-conceptions. For so many years there was this notion that ADHD was a disorder of childhood that that was the end of it. We never looked at adults because of preconceived notions. We’re now at the point where young adults are coming back to their old pediatricians and saying, “Hey, Doc, I still need some of that medication.”
As ADHD children have grown, we’ve started seeing this adult ADHD coming on. We’re now looking more closely into a rich, complex, and highly co-morbid condition that really makes a difference to people’s lives. We’ve known for quite some time that having ADHD as a kid is a predictor of other kinds of emotional problems in adulthood, depression and anxiety disorders, substance use disorders and so forth. We’re now coming to realize that it’s also a risk factor for this broader and subtler ADHD variant that we hadn’t recognized until recently, and then once we see it more clearly than we have in the past, it could well be that new treatment options present themselves that we haven’t appreciated before. That of course is the holy grail for us moving forward in understanding the full life spectrum of ADHD.